Case Study: 15-Year-Old Domestic Shorthair Cat with Multiple Myeloma

Annabel Travers
BVMedSci (Hons), BVM BVS (Hons), DipACVP (Clin Path), MRCVS
Board Certified Clinical Pathologist
Signalment
A 15-year-old domestic shorthair cat, neutered male, presented to the clinic for evaluation of lethargy, weight loss, and reduced appetite. The cat had a known history of heart failure, which was managed with medication. During physical examination, mild dehydration was noted along with pallor of the mucous membranes. There was no evidence of lymphadenopathy, however osteolytic bone lesions of the spinal vertebrae were present on radiography.
Clinical Presentation and Laboratory Findings
The initial laboratory workup revealed several abnormalities. The cat had a marked hyperglobulinemia with a globulin level of 160 g/L, accompanied by a markedly low albumin-to-globulin (AG) ratio of 0.1, indicating a hyperproteinaemia state driven by an elevated globulin fraction. Blood tests also revealed moderate azotaemia, which could be a result of renal impairment either due to hyperproteinaemia or as an independent comorbidity in this older cat. Additionally, a moderate neutrophilia was noted, alongside mild non-regenerative anaemia, which is often associated with chronic inflammation or neoplasia.
Cytologic Findings
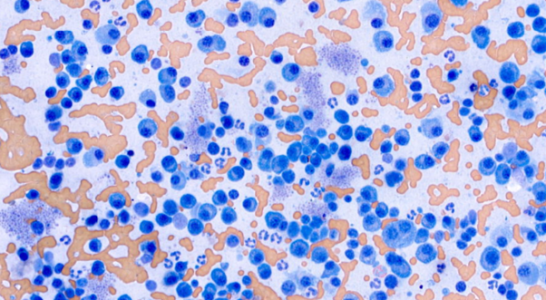
Fine-needle aspirates were taken from the liver and spleen to further investigate the hyperglobulinemia and other laboratory abnormalities. Cytologic evaluation of the spleen revealed a large population of discrete cells with moderate pleomorphism, eccentric nuclei, and deeply basophilic cytoplasm. These cells exhibited moderate anisocytosis and anisokaryosis and occasional binucleation. Occasional mitotic figures were seen. A similar cytologic picture was observed within the liver. The cytological findings were consistent with plasma cell neoplasia.
Diagnosis and Discussion: Plasma Cell Neoplasia in Cats
Multiple myelomas are plasma cell neoplasms that originate in the bone marrow and infiltrate other organs, whilst solitary plasma cell tumours in organs other than bone marrow are plasmacytomas. Neoplastic plasma cells secrete abnormal immunoglobulins which appear as a monoclonal spike on protein electrophoresis. Diagnostic criteria for multiple myeloma, initially outlined by MacEwen and Hurvitz in 1977 for dogs, require at least two of four specific indicators: (1) paraproteinemia or monoclonal gammopathy, (2) radiographic evidence of osteolytic bone lesions, (3) Bence Jones proteinuria (abnormal immunoglobulin light chains in urine), and (4) greater than 5% neoplastic plasma cells in the bone marrow. In this case, cytologic evidence of an atypical plasma cell proliferation in both the liver and spleen, alongside a marked hyperproteinaemia and presence of osteolytic lesions is strongly suggestive of multiple myeloma, although bone marrow samples were not obtained for confirmation.
Clinical signs of multiple myeloma are non-specific and can include lethargy, anorexia and weight loss. Initial work up may reveal renal impairment, anaemia and osteolytic lesions. However, osteolytic bone lesions, a hallmark of multiple myeloma in dogs, are less frequently observed in cats. An azotaemia (as seen in this case) may reflect existing renal compromise or reduced glomerular filtration rate secondary to hyperviscosity syndrome.