Case of the Month: Feline Cowpox

Taiana Costa Kirkham
MV, Mphil, PhD, Dipl.ECVP, MRCVS
Board-certified Anatomic Pathologist
Leo, 1 year old male Domestic Shorthair cat
Clinical history
Leo presented with swelling of the left forepaw characterised by the presence of multiple cutaneous lesions with scabs and poor skin integrity.
Histology
Three punch biopsies of haired skin were submitted for histopathological examination. These samples showed extensive epidermal ulceration, and severe epidermal and dermal necrosis, characterized by the presence of large amounts of amorphous eosinophilic material, pyknotic and karyorrhectic cellular debris, degenerate and viable neutrophils, fibrin and haemorrhage. There was marked inflammation extending from the ulcerated tissue into the deep dermis comprising large numbers of neutrophils and eosinophils, moderate to large numbers of macrophages often palisading around necrotic and disrupted hair follicles which faded in the face of necrosis and the associated inflammatory infiltrates (Figure 1). Fragments of free hair shafts were frequently entrapped within the inflamed tissue. There was also mild to moderate oedema and proliferation of endothelial cells and fibroblasts in the background.
In the superficial disrupted tissue there were multiple residual islands of follicular infundibular epithelium embedded within the areas of necrosis. Keratinocytes often showed variably-sized bright eosinophilic intracytoplasmic inclusions, consistent with cowpox A-type inclusion bodies (Figure 2).
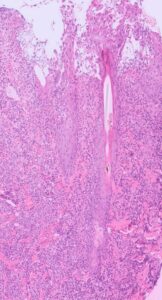
Photomicrograph showing severe ulcerative and necrotising dermatitis (HE, 10x).

Figure 2: Photomicrograph showing large numbers of variably-sized bright eosinophilic intracytoplasmic viral inclusion bodies (arrows) within keratinocytes, consistent with cowpox A-type inclusion bodies (HE, 40x).
Interpretation
Dermatitis, ulcerative, necrotising, neutrophilic, eosinophilic, histiocytic to pyogranulomatous, multifocal, subacute, severe, with intralesional eosinophilic intracytoplasmic inclusion bodies in keratinocytes – consistent with cowpox A-type inclusion bodies.
Molecular testing
A fresh skin biopsy was also submitted to our lab for Orthopoxvirus qPCR, and yielded a positive result, with a Ct value of 15.5. Ct values typically range from 15-40, and the higher the Ct value, the lower the amount of DNA present in the sample. Therefore, these results indicate a high level of Orthopoxvirus DNA in the sample submitted.
Comments
Histology of the samples of haired skin submitted captured a severe ulcerative and necrotising dermatitis (Figure 1). Residual hair follicles were observed, and keratinocytes showed moderate to large numbers of variably-sized and bright eosinophilic intracytoplasmic inclusion bodies – consistent with cowpox A-type inclusion bodies (Figure 2). In this case, cowpox virus infection was presumptively diagnosed based on the presence of characteristic intracytoplasmic inclusion bodies, and was confirmed using Orthopoxvirus qPCR.
Ulcerative and necrotizing dermatitis in cats can also be attributed to feline herpesviral dermatitis, resulting from Felid herpesvirus 1 infection. It’s essential to consider this as a potential alternative diagnosis, particularly in cases where eosinophilic intracytoplasmic inclusion bodies are absent, and if the mixed dermal inflammatory infiltrate includes eosinophils.
What is cowpox?
Cowpox is an infection caused by cowpox virus (genus Orthopoxvirus), considered a re-emerging zoonotic pathogen and a public health threat due to increasing numbers of cases in humans and animals in Europe over the past decade, including within the United Kingdom. In addition to cattle, cowpox virus may infect cats, dogs, and various non-domestic species. Serological studies have established that the most likely reservoirs of CPXV in Great Britain are bank voles (Myodes glareolus), short-tailed field voles (Microtus agrestis) and, to a lesser extent, wood mice (Apodemus sylvaticus). The highest seasonal incidence of feline cowpox is from late summer to autumn, corresponding with the peak size of rodent populations.
The majority of feline cowpox cases feature a solitary primary cutaneous lesion, typically found on the head, neck, forelimb, or paws. During the viraemic phase, which occurs 1-3 weeks after the appearance of the primary lesion, secondary skin lesions emerge widely. Initially, the skin lesions present as small papules, which gradually enlarge into nodules and subsequently ulcerate, forming craters and crusts. Vesicles are seldom observed, particularly on the oral mucosa and inner pinna. Generally, full recovery is observed within 4-5 weeks.
Atypical cutaneous cowpox virus infection has also been observed in cats, presenting with skin lesions on the distal limbs characterised primarily by oedema, hyperaemia and plaque-like lesions, rather than the typical ulcerated papules. Feline cowpox can also manifest in a mucocutaneous form and, in rare instances, can become systemic, replicating in internal organs, particularly the lungs and upper gastrointestinal tract, often resulting in a fatal outcome. Rare cases of fatal necrotizing pneumonia without the presence of typical skin lesions have also been reported.
Cowpox has rarely been reported in dogs and other domestic species. However, non-domestic species are also susceptible, with exotic felids, particularly cheetahs, being at high risk of developing systemic disease.
Zoonotic potential
Cowpox is a rare zoonotic disease that poses a significant risk for immunocompromised individuals, including children, elderly and pregnant women. Approximately 50% of human cowpox cases are associated with feline cowpox infections.1 Therefore, pet owners and veterinary staff who come into direct contact with infected cats are advised to seek medical attention if they develop skin lesions suggestive of cowpox.
References
1Lawn, R. (2010) Risk of cowpox to small animal practitioners. Veterinary Record, 166: 631-631. https://doi.org/10.1136/vr.c2505