Here at the VPG, we encounter dozens of new, interesting and occasionally confusing cytological cases from your patients every day – our interpretations are greatly improved when we work as a team with our clinicians to get the best out of our samples. With that in mind, here is some advice on some things to consider (and some things to avoid) when sending in cytological samples.
Labelling slides
We process hundreds of slides a day across our sites. Accurate labelling helps avoid any problems during processing and staining, as well as saving time and avoiding confusion when we examine them. Some advice:
- Label the submitted slides with the patient’s name, surname, and brief description of the sample location.
- Label each slide individually – unlabeled slides in labelled slide holders are very hard to identify once removed from the box (although, ideally, label the slide holders too).
We find that felt pen written on slides can fade in transit or erased during the staining process; ink pen occasionally will be too. Sticky labels can also be lost on transit or during processing. Pencil written on frosted glass is preferable and unlikely to be lost. Scratching details onto a slide with an engraving tool can also work, although it can be time consuming for the clinician and hard to read.

**Fig 1 – A well-labelled slide with pencil on frosted glass**
Labelling fluids
- Label every sample tube with the patient’s name and site of the sample (especially important when multiple fluids are submitted, or fluid is submitted alongside blood). The date of sampling is also useful for fluid samples to help us assess deterioration since sampling.
- Where possible, submit direct fresh in-house smears as well as fluid (although this is largely unhelpful for poorly cellular fluids such as CSF or respiratory samples).
- When in-house smears are included with a specimen, clearly label whether the preparation was smeared directly from the sample (direct) or whether the sample was concentrated prior to preparing the smear (concentrated). This makes it much easier for the pathologist to assess the cellularity of the sample.
Submission form
We understand the many demands on your time in practice, but correctly filling in a submission form will lead to a quicker result and often a more relevant report. We have received submissions missing any (or all!) of the information discussed below, and in each case the reporting of the sample has been slower as a consequence.
Patient and practice details
Include all salient details of the patient with the submission form – this includes name, age, species, breed, date of sampling, sex and neutering status – as well as the submitting practice and the clinician involved. Where some details are ambiguous or have recently changed (for instance, a sample taken from a patient that was neutered at the same time as sampling) then it helps to briefly explain this in the history section.
History
A concise and relevant history is extremely important for submissions; cytology is a subjective discipline, and the context in which samples are taken and examined is important. Samples with no history at all are likely to lead to a more equivocal report or a phone call from the lab requesting more details, delaying the report. Similarly, including unedited clinical notes for patient’s last few weeks, months or years can lead to relevant details being missed when sandwiched between pages of clinical notes, flea treatment and wormer sales.
The most helpful details to include with a submission are as follows:
- Precise location of sites sampled (see below for some notes on anatomy)
- Reason for sampling (e.g. lesions found on imaging, persistent enlargement, history of neoplasia elsewhere)
- Gross appearance (or appearance on imaging/features on palpation for internal masses) e.g. hairless, diffuse versus discrete mass, hyper/hypoechoic, colour, texture, attached versus mobile
- Other potentially relevant clinical findings (e.g. marked hyperglobulinaemia, hypercalcaemia, masses elsewhere not sampled)
- Details from previous history which may be relevant (e.g. previous mast cell tumour, currently on chemotherapy, bouts of pancreatitis, history of trauma in the sample location)
It can also be useful to include the differential diagnoses you are most suspicious of or ask any clinical questions that you are particularly interested in, which can help focus the pathologist on the details most relevant to your case (e.g. ‘Concerned for mast cell tumour’; ‘Is this swelling a lymph node?’; ‘Suspect hepatic nodular hyperplasia but want to rule out neoplasia’ etc.)
Anatomy
Medical terminology (as well as providing useful face-saving terms such as ‘idiopathic’ and ‘iatrogenic’) furnishes clinicians with detailed ways of describing the precise location of lesions. It is a shame to allow these elegant terms to go to waste by instead using ambiguous language which can lead to confusion and misinterpretation. Here are some terms that will often need clarification (many don’t need to be completely avoided, but further details to locate lesions more accurately will be helpful):
Neck – this may seem like a precise term, but it actually covers everywhere from the thoracic inlet to the submandibular region, and says nothing about whether a lesion is dorsal, ventral, or lateral. ‘Neck lump’ could represent anything from a thyroid carcinoma to a sarcoma involving the spinous processes of the cervical vertebrae.
Throat – again, this may seem like a precise location, but actual covers a wide anatomical area, and, in isolation, does not make it clear whether a lesion is present within the oropharynx, larynx or the subcutaneous or cutaneous tissues surrounding them.
Rump – another term which can refer to large areas of a patient, from the dorsal pelvis, pelvic limbs, tail base or anal mass.
Bum – another non-specific term, although this one makes my kids laugh so has slightly more merit.
Abdominal/thoracic – remember to include details of whether lesions are intraabdominal/thoracic, or extraabdominal/thoracic. ‘Abdominal mass’ is more ambiguous than it appears at first.
Cervical – frustratingly, despite me waxing lyrical above about the elegance of anatomical terms, ‘cervical’ can actually refer to two separate anatomical locations: the cervical spine, or the cervix (it comes from the Latin for ‘neck’ but is often applied to general narrowing of tissues). Regardless, remember to clarify which location you are referring to with submissions.
Subcutaneous versus cutaneous – these are precise terms (as are their synonyms dermal and subdermal) but are often misused, especially as it can be challenging to tell the difference in some diffuse or invasive lesions. Cutaneous masses are usually visible on the skin’s surface or are clearly palpable just underneath it – if the skin is lifted, then a cutaneous mass lifts as well. In contrast, ‘subcutaneous’ masses are present beneath the surface of the skin and are only visible when they deform the overlying skin. The skin is generally mobile over subcutaneous masses except for lesions which have invaded the cutaneous layer, and when the skin is lifted, a subcutaneous mass should remain in its original position.
For lesions where it is not entirely clear whether the mass is cutaneous or subcutaneous, record this difficulty in classifying on the submission form.
Side/Dorsum/Ventrum – ‘side’ leads a lot to the imagination, encompassing both forelimbs, the neck (a vague term in itself), the thoracic and abdominal wall and can even be applied to mammary glands. ‘Dorsum’ and ‘ventrum’ are similarly non-specific when used alone.
Foot – this is relatively specific, but more information to clarify if a lesion is on a digit, interdigital, on a pad or in the nail base is helpful as it may affect the interpretation.
Packaging
Even when the sample has been successfully taken, labelled, and a concise and relevant history has been included, mistakes in packaging can significantly affect the quality of specimens and the chance of diagnosis. Here are the most common pitfalls to avoid:
Do not pack cytology with histopathology – unfortunately, cytology specimens are very sensitive to formalin fumes; even limited exposure has a significant effect on the quality and preservation of samples. Cytology exposed to formalin has a washed-out appearance, with erythrocytes and many nucleated cells faded, ruptured and often stained an unpleasant greenish colour. This can ruin an otherwise diagnostic sample.
To avoid the risk of this, submit histopathology and cytology specimens separately.

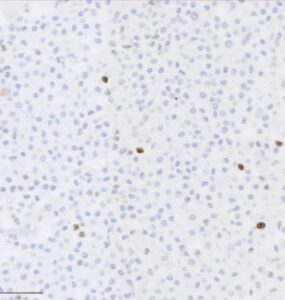
**Fig 2 – Greenish discolouration of red blood cells due to formalin fumes**
Do not package wet slides – when slides are placed into slide holders before they are fully dry, the condensation results in ‘drying artefact’ – it leads to rupture of many cells and markedly reduces the quality of samples. The telltale sign of drying artefact is red cells reduced to spiky haemoglobin crystals and this can, again, ruin a perfectly good sample.
To avoid this, ensure that slides are completely dry before packaging. For some samples (such as synovial fluid preparations), using a hairdryer on the cool/gentle setting can help to speed up the drying process.

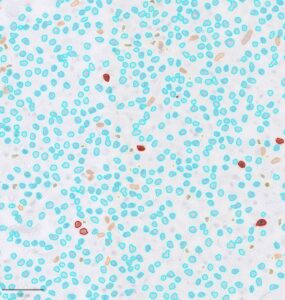
**Fig 3 – Haemoglobin crystal formation due to packaging slides while still wet**
Avoid submitting slides with coverslips– these need to be removed to allow us the stain the samples. Removing them is time-consuming, sometimes difficult, and sometimes damages the specimen.
Avoid prestaining slides all submitted slides – we love cytology, and so quite understand that once you have taken a sample, you are interested in having a look yourselves. As pathologists, however, we are creatures of habit and ritual (notably manifested in our complicated tea runs), and we are accustomed to our modified Wright’s stain. Although pre-staining will not ruin preparations, it alters the staining properties of the slides and can make certain conditions more challenging to identify (for example, mast cell granules may not stain well, and nuclear features can be accentuated on pre-stained slides). Pre-staining, as with many things in life (except cheese) is fine in moderation, but it is helpful to leave some cellular slides unstained for us.
Take home messages
- Label individual slides as well as slide holders, ideally with pencil on frosted glass
- A concise and relevant history will help speed up the process and improve chances of a diagnosis
- Use precise anatomical terms (avoid ‘neck’, ‘throat’, ‘bum’)
- Package cytological and histological specimens separately
- Do not package slides when they are still wet
- Avoid submitting slides with coverslips on
Download your free Cytology Submission Checklist
Ensure every sample is prepped perfectly – print and keep this handy reference in your practice.